
INTRODUCTION
After cataract/refractive surgery, an increasing number of patients, mainly younger than 65 years, demand very good intermediate vision, as well as near vision, which is important at arm’s length or longer [1]. In today’s world, intermediate vision is even more crucial than near for performing daily tasks such as using mobile phones, computers and tablets. An interesting option for such patients is trifocal intraocular lenses, which provide better intermediate vision in comparison with bifocals without impairing near and far visual acuity (VA) [2]. Currently, several trifocal diffractive intraocular lenses (IOLs) are available, including FineVision (PhysIOL SA), AcrySof IQ PanOptix (Alcon) [3], Acriva Reviol Tri-ED 611 (VSY Biotechnology), Versario 3F (Bausch + Lomb), and AT LISA tri (Carl Zeiss AG) [3–5].
To date, in the available literature there is only one study describing 3-month standard visual outcomes after implantation of new low addition (+3 diopters, D) Versario 3F (Bausch + Lomb) trifocal IOLs [6], and the results were promising. It is known from the results of other studies that the neuro- adaptation process lasts at least 6 months and has an important role in the improvement of visual outcomes and reduction of unwanted effects such as glare and halo after implantation of multi-focal IOLs [6–10]. Hence, we decided to analyze six-month visual outcomes, patient satisfaction, and complications after bilateral implantation of Versario 3F trifocal intraocular lenses.
MATERIAL AND METHODS
Study design and patients
The prospective study included 20 patients (40 eyes) – 13 women and 7 men – who underwent uneventful, bilateral, sequential cataract surgery in the 2nd Department of Ophthalmology, Pomeranian Medical University in Szczecin, Poland. The patients were interested in spectacle independence and were informed about the advantages and disadvantages of multifocal IOL implantation. The study adhered to the Declaration of Helsinki and was approved by the local ethics committee. Written consent was provided by all patients.
Inclusion and exclusion criteria
The inclusion criteria for multifocal IOL implantation included age 55–70 years, bilateral cataract, pupil size 3–6 mm in dim light, preoperative corneal astigmatism less than 0.75 D, hyperopic presbyopia, patients’ motivation for spectacle independence, tolerant patients, willing and able to comply with scheduled visits.
Exclusion criteria for multifocal IOL implantation included ocular diseases other than cataract, unrealistic visual expectations related to lifestyle or profession, professions requiring very high visual precision (e.g., pilots, professional drivers, architects), satisfaction with reading glasses, and age over 70 years due to potential difficulties with neuroadaptation to new optical conditions. Additional exclusion criteria included psychiatric disorders, dissatisfaction with progressive spectacles, and a history of stroke or dyslexia, as well as type A personality traits (perfectionism).
Intraocular lens
The Versario 3F intraocular lens (Bausch + Lomb) is a tri-focal IOL made of hydrophilic acrylic material (25%) with a hydrophobic surface. It features a 6.0 mm, diffractive, biconvex, aspheric optic, an overall diameter 11 mm, a plate- haptic, microincision cataract surgery (MICS) (1.8 mm) design, angulation 0°, with spherical diopter power from 0.00 to +32.00 D in 0.5 D increments. The refractive index is 1.46. The Versario 360° square edge design blocks epithelial cell migration into optic area, preventing early posterior capsule opacification. The near power of this lens is +3.00 D, and the intermediate power is +1.5 D at the IOL plane. The manufacturer’s A-constant for this IOL is 118.6. The Versario 3F IOL is implanted using the Bausch + Lomb Injector system (Viscojet TM BIO 1.8). The innovative smooth-step design of the Versario 3F IOL is intended to minimize unwanted halo effects, glare, and light scatter, while maintaining high contrast sensitivity under scotopic and mesopic conditions.
Preoperative and postoperative examination
Preoperatively, all patients underwent a comprehensive ophthalmological examination, including uncorrected and best corrected distance VA, subjective refraction, corneal topography (Atlas 9000, Carl Zeiss Meditec AG) slit lamp biomicroscopy of the anterior and posterior segments of the eye using Volk lenses, Pascal tonometry, and biometry (IOLMaster 500, Carl Zeiss Meditec AG).
Six months after binocular surgery, the clinical evaluation included the following tests: binocular uncorrected distance visual acuity (UDVA) measured using the logarithm of the minimum angle of resolution (logMAR) Early Treatment Diabetic Retinopathy Study (ETDRS) chart at 4 m; uncorrected near visual acuity (UNVA) at 40 cm; uncorrected intermediate visual acuities (UIVA) at 60, 70, 80 cm; binocular defocus curve with the ETDRS chart positioned at 6 m in photopic conditions [the change in VA after addition of 0.5 D increments at each step towards hyperopia (0 +1.5 D) and myopia (0 –3.0 D)], binocular photopic (85 cd/m2) and mesopic (3 cd/m2) distance (2.5 m); binocular photopic near (35 cm) contrast sensitivities at 2.5 m (1.5, 3, 6, 12, and 18 cycles/degree) using the Contrast Sensitivity Vision-1000 and the Functional Acuity Contrast Test (F.A.C.T.); spectacle independence; subjective symptoms (glare and halo); patient satisfaction evaluated with the modified Visual Function Questionnaire (VFQ-25) [11]; and postoperative complications.
Surgical technique
The phacoemulsifications (Stellaris – Bausch & Lomb) were performed by the same surgeon (W.L.) under topical (Alcaine) and intraocular (1% lidocaine) anesthesia. Versa-rio 3F lenses were implanted through a mean 1.8 mm clear corneal incision. The capsulorhexis was approximately 5 mm and was performed using the Mile High Ophthalmic 5.0 Ophthalmic Caliper LLC.
After cataract removal, the IOLs were inserted in the capsular bag. The IOL power was calculated using optical bio- metry (IOLMaster, Carl Zeiss Meditec, Jena, Germany) and the SRK/T or Hoffer Q formulas. The target refraction was emmetropia.
Postoperatively, all patients were prescribed eye drops of moxifloxacin, prednisolone, and nepafenac for the first 4 weeks.
RESULTS
The study group consisted of 40 eyes of 20 patients. Mean age was 64.3 ±6.4 years (range 55 to 70 years). Table I shows binocular uncorrected visual acuities for distance, interme- diate, and near vision after surgery.
Table I
Binocular logarithm of minimum angle of resolution (logMAR) visual acuities after surgery
| Visual acuity | Distance | Mean ±SD (logMAR) |
|---|---|---|
| UDVA | 4 m | –0.12 ±0.08 |
| UNVA | 40 cm | +0.12 ±0.12 |
| UIVA | 60 cm | +0.07 ±0.10 |
| UIVA | 70 cm | +0.05 ±0.11 |
| UIVA | 80 cm | +0.07 ±0.09 |
UDVA was better than –0.1 logMAR in 30% of patients. Very good results of more than –0.2 logMAR were achieved by 60% of patients. UNVA was 0.1 logMAR in 50% of patients. UIVA in 40% of patients was 0.1 logMAR, and in 40% of patients was 0.0 logMAR or better.
Figures 1, 2, and 3 present data of our VA in comparison with data of Fernández et al. [6].
Figure 1
Comparison of binocular uncorrected distance visual acuity between our group of patients (black) and that of Fernández et al. [6] (grey)
VA – visual acuity
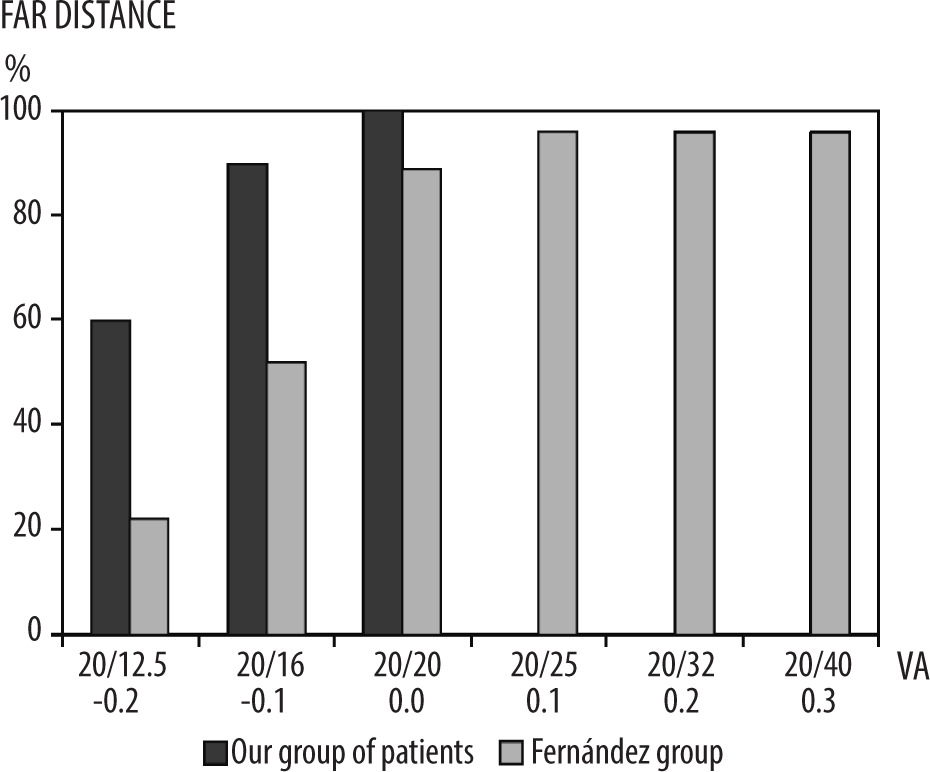
Figure 2
Comparison of binocular uncorrected intermediate visual acuity between our group of patients (black) and that reported by Fernández et al. [6] (gray)
VA – visual acuity
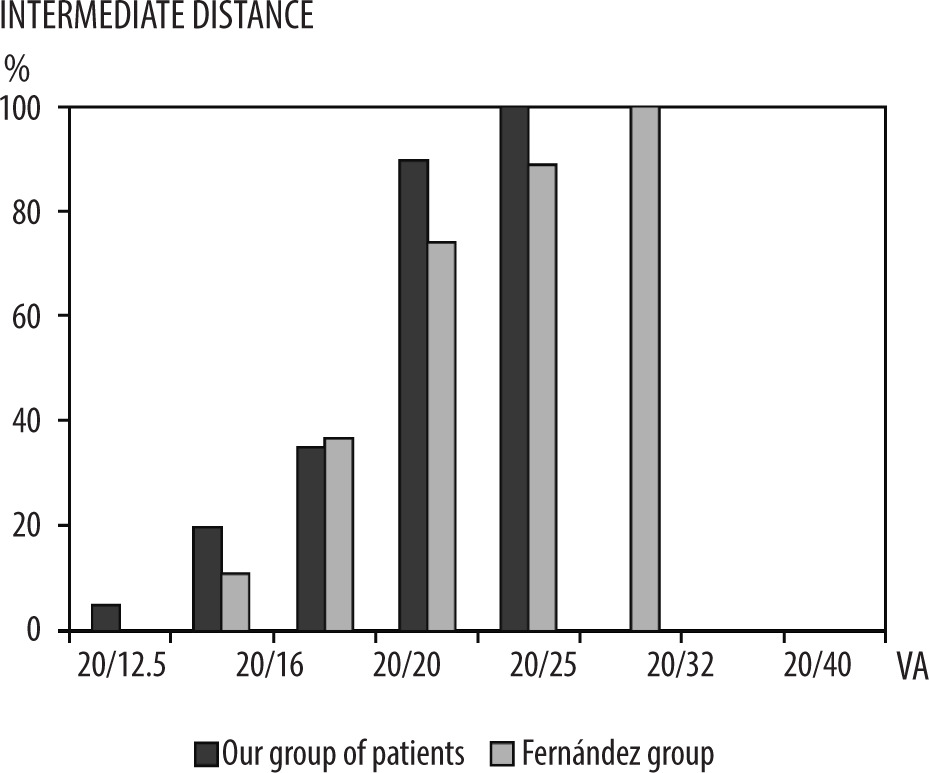
Figure 3
Comparison of binocular uncorrected near visual acuity between our group of patients (black) and that reported by Fernández et al. [6] (gray)
VA – visual acuity
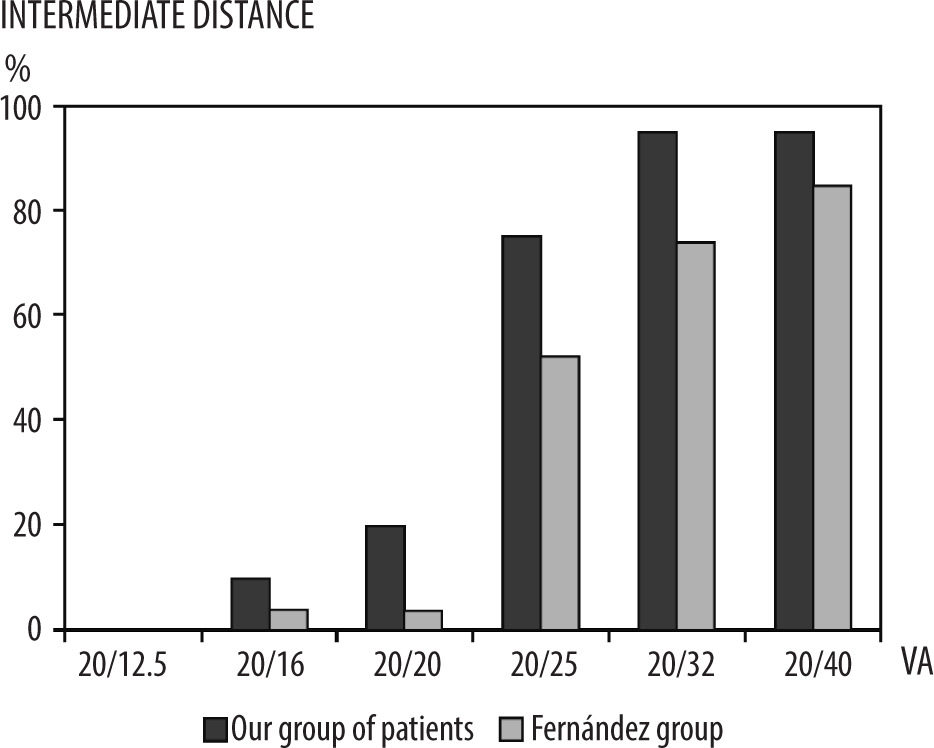
Figure 4 shows the defocus curve between –3.0 and +1.0 D, which was evaluated using a depth of focus method, in comparison with the results of Fernández et al. [6]. The results were correlated with the subjective perception of near and intermediate vision.
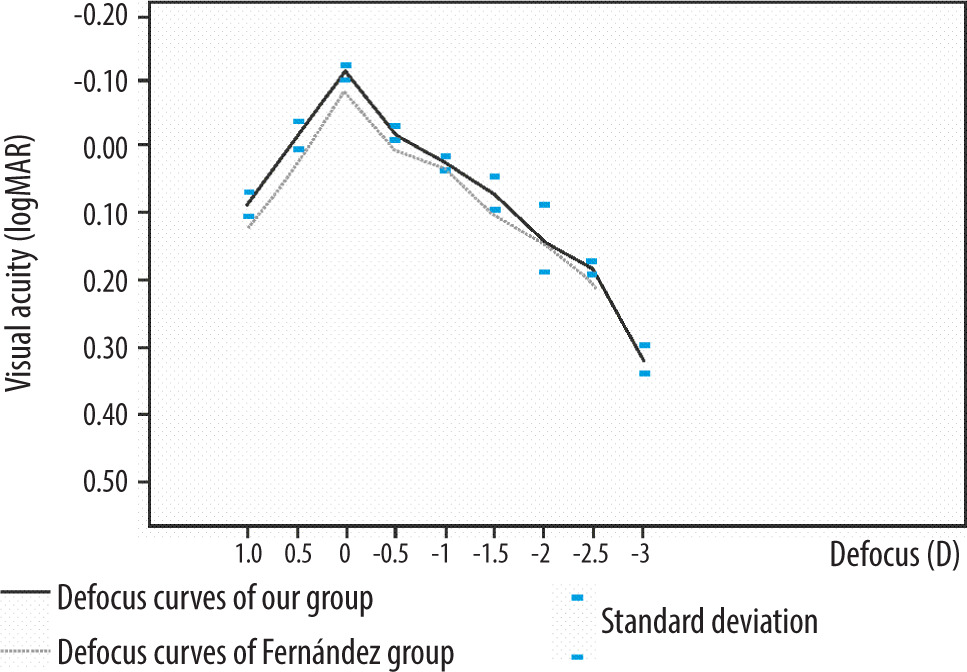
Figure 5 shows contrast sensitivity results for binocular vision at far, intermediate, and near distances in comparison to the age-matched healthy control range.
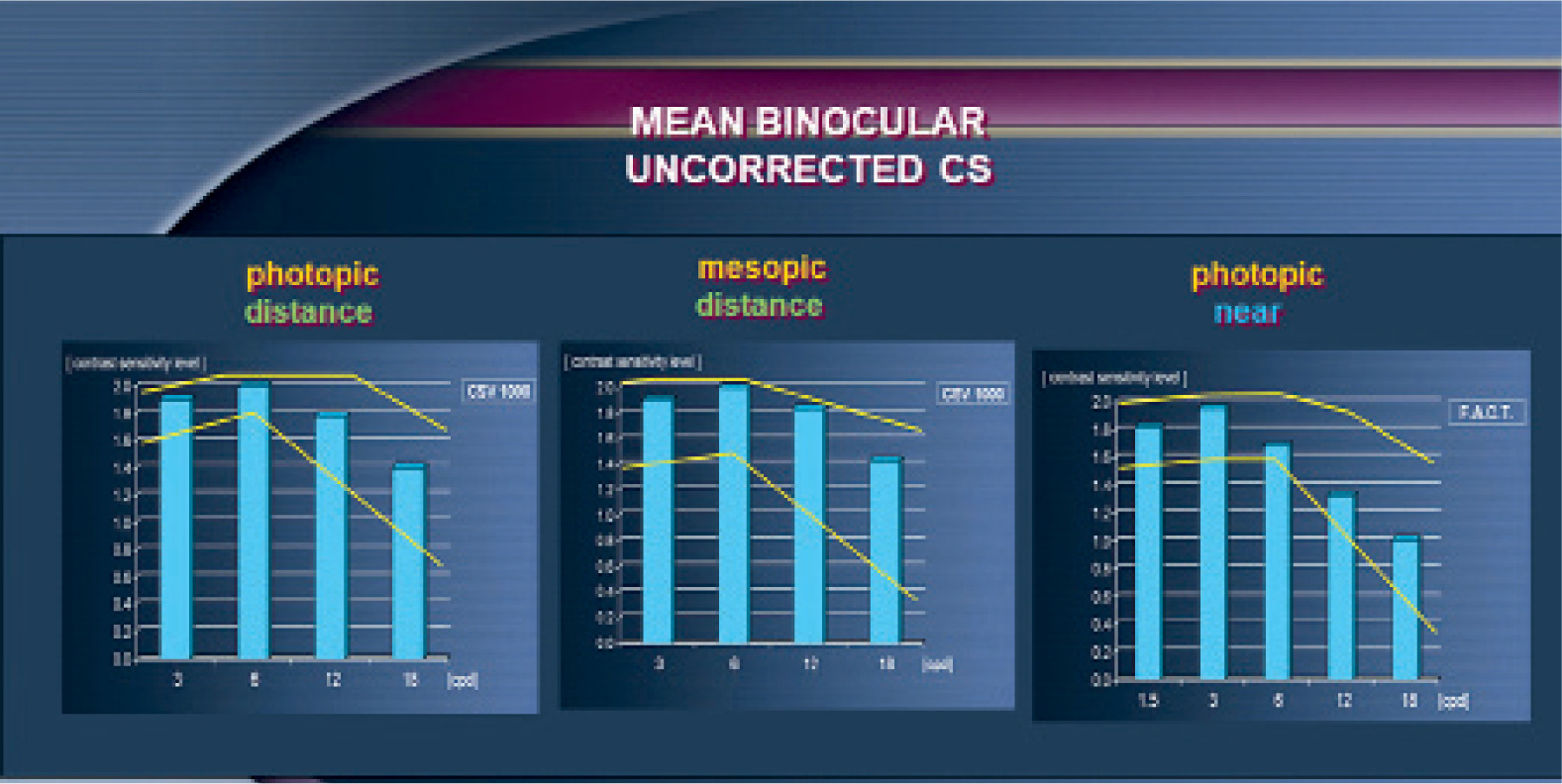
Patients had satisfactory contrast sensitivity at 1.5, 3, 6, 12, and 18 cycles/degree, being within the normal range values found in the F.A.C.T.
Table II presents the results of patient satisfaction in the modified VFQ-25 test. Total spectacle independence was achieved in 100% of the Versario group. General VA was very high (1.47). Also, very good results for all important activities were observed. No patient experienced severe optic phenomena.
Table II
The results of patient satisfaction in the modified VFQ-25 test (binocular, unaided vision)
There was no need for refractive lens exchange in any patient, and all patients stated that they would be willing to repeat surgery with the same IOL.
DISCUSSION
The presented visual function outcomes six months after implantation of Versario intraocular lenses (IOLs) were promising and comparable with data presented by Fernández et al. [6].
In our study, very good distance VA of –0.12 logMAR was achieved after binocular implantation of Versario lenses. The results were slightly better compared to those obtained by Fernández et al. [6] using the same trifocal Versario IOL (0.02 logMAR) and other trifocal IOLs: LISA tri 839MP (–0.03 to 0.08 logMAR), PanOptix (0.07 logMAR), Acriva Reviol (–0.05 logMAR), FineVision (0.03 to 0.12 logMAR) [3, 6, 7]. Possible explanations of our better results in comparison to other authors using different trifocal IOLs are the small number of cases, the precise patient selection for pre- mium IOLs, and the design of the Versario IOL.
In our study, binocular UNVA (0.12 logMAR) was better than that reported in the study by Fernández et al. [6] (0.24 logMAR), probably due to a longer neuroadaptation period. The VA values reported in the above-mentioned studies were comparable with those obtained with other trifocal IOLs: AT LISA tri (0.11–0.22 logMAR), PanOptix (0.17 logMAR), Acriva Reviol (0.06 logMAR), and FineVision (0.04–0.21 logMAR) [7, 9].
Nowadays, patients visiting ophthalmological clinics expect very good vision for intermediate distances because of common usage of electronic devices such as computers, laptops and dashboards, and car navigation. The results of intermediate vision of Versario lenses in our study suggest that these lenses cover the expectations of such patients. Our results were very satisfactory for 3 measured distances: 60, 70, and 80 cm. Our result was 0.05 logMAR for the distance 70 cm. It was comparable to AT LISA tri and Acriva Reviol. The result reported by Fernández et al. [6] for the Versario IOL was worse (0.19 logMAR). We believe that, similar to near vision, the differenc es in UIVA between our study and that reported by Fernández et al. [6] are likely due to a longer neuroadaptation period [8].
The distance uncorrected binocular photopic and mesopic contrast sensitivities (CS) and binocular uncorrected near photopic CS were within normal limits, and this is the first information concerning CS after implantation of Versario lenses. No differences compared to other trifocal IOLs and extended depth of focus (EDOF) lenses were found. CS under both photopic and mesopic conditions were similar among the AT LISA, PanOptix, FineVision, and the EDOF IOL [12].
The results of the defocus curve confirm very good results for distance and intermediate vision, and the shape of the defocus curve was comparable to the Fernández et al. [6] study.
Analysis of spectacle independence is one of the important features describing the quality of premium IOLs. In our study, all patients after implantation of Versario IOLs were spectacle independent, which suggests high quality of this lens. The frequency of patients with total spectacle independence has a better result (100%) than all three other IOLs (89%, 90%, and 86% in the PanOptix, FineVision, and Symfony groups, respectively) [13]. Overall, 86 to 90% spectacle independence was achieved.
We believe that total spectacle independence was obtained primarily as a result of precise selection of the patients for this type of IOL. The second cause of total spectacle independence is precise power calculation. In all patients, postoperative refractive errors were no more than +/–0.5 D. The final explanation is the small number of patients included in our study.
The next important parameter describing VA of premium IOL is analysis of patient-reported visual function using a standardized questionnaire. Nowadays, it is very difficult to compare visual function (VF) data across studies, because there are no international standards for assessing quality of vision using VF questionnaires. In our study, a modified VFQ-25 test was used. General satisfaction was very high (95%), in line with Fernández et al. [6].
Separate analysis of distance, near, and intermediate visual performance also showed very high outcomes, with a mean result of 1.47. In all functional activities described in detail in Table I, our patients achieved very good outcomes.
General satisfaction was similar to that obtained with other trifocal IOLs. Patient satisfaction at far distance was about 96.3% according to Fernández et al. [6], and 94% with AT LISA tri (Mendicute group), compared to 95% in our patients [14].
Halo and glare were the most frequently reported visual disturbances (70% and 50% for PanOptix and Symfony according to Mencucci et al. [15]), although the symptoms were rated mostly as mild or, at least, as not disturbing by the patients [16].
A disadvantage of multifocal IOL implantations is presence of photopic phenomena – glare and halo caused by overlapping imagines. In our study, in 15–20% of patients glare or halo was experienced, but fortunately with a low level of perception, which is important, as no patient wanted to exchange the lens because of photopic phenomena. The frequency and severity of unwanted effects were within the range of frequency or severity of photopic phenomena described by others implanting IOLs.
Halos, glare, and difficulty in night time driving are side effects of patients with multifocal intraocular lenses (MIOLs). In the majority of patients, photopic disturbances decreased with time and did not impact their lives. This phenomenon has been termed neuroadaptation, wherein patients require a certain postoperative period to adjust to the retinal images, and this is frequently observed with MIOLs. The Versario lens was comparable to different trifocal IOLs. It can be classified as a trifocal EDOF IOL because of the performance between EDOF IOLs and medium-high addition trifocal IOLs [6].
CONCLUSIONS
Bimanual MICS with implantation of Versario lenses is a safe and effective method for patients who want to be spectacle independent at multiple distances. Comparison of visual outcomes after implantation of the Versario lens with other trifocal IOLs supports the conclusion that such lenses can be offered and proposed equally with other multifocal lenses in patients who want to be spectacle independent.







