
INTRODUCTION
Acute retinal pigment epitheliitis (ARPE) is a self-limiting inflammatory disorder of the retina [1]. The disease was first described in 1972 by Krill and Deutman [2]. Roy et al. [3] described ARPE as a subtle macular lesion with macular pigment epithelial alteration in the fundoscopy. Usually it affects only one eye; however, there are also bilateral cases described in the literature. Sex does not influence the incidence of occurrence: females and males are equally affected. Age is reported to be associated with the disease incidence: mostly young people are affected, in the range from 10 to 40 years old. ARPE is described as a self-limiting disease which can retreat autonomously with good visual recovery [1, 4]. The exact etiology and pathogenesis of ARPE remain unknown. The literature includes reported cases of ARPE associated with either an episode of Coxsackie A virus infection, coronavirus disease 2019 (COVID-19), bisphosphonate therapy, or vaccination against COVID-19 [5]. Al-Nofal et al. [6] described visual impairments in ARPE as a paracentral group of 2–4 grey spots in the macular region with a surrounding yellow or white halo zone. Compared to other macular diseases or central chorioretinitis, it has a good prognosis; therefore, for optimal patient management and comfort, an accurate diagnosis is crucial. Fundoscopy, optical coherence tomography (OCT), and fluorescent angiography are essential to avoid unnecessary treatments [7]. White dot syndromes should be considered in the differential diagnosis of ARPE, with particular reference to acute posterior multifocal placoid pigment epitheliopathy, because of the similar features.
CASE REPORT
A 36-year-old male patient presented to our clinic’s emergency department with left eye visual disturbances. He had been undergoing treatment for depression, transitioning to vortioxetine one month previously. Additionally, he had a history of seasonal grass pollen allergy. His family and medical histories were unremarkable. A week earlier, he had sought consultation with a local ophthalmologist due to rapid deterioration of vision in his left eye following a mild infection, accompanied by a temperature up to 38°C. At that time, his left eye visual acuity was noted to be 1/50.
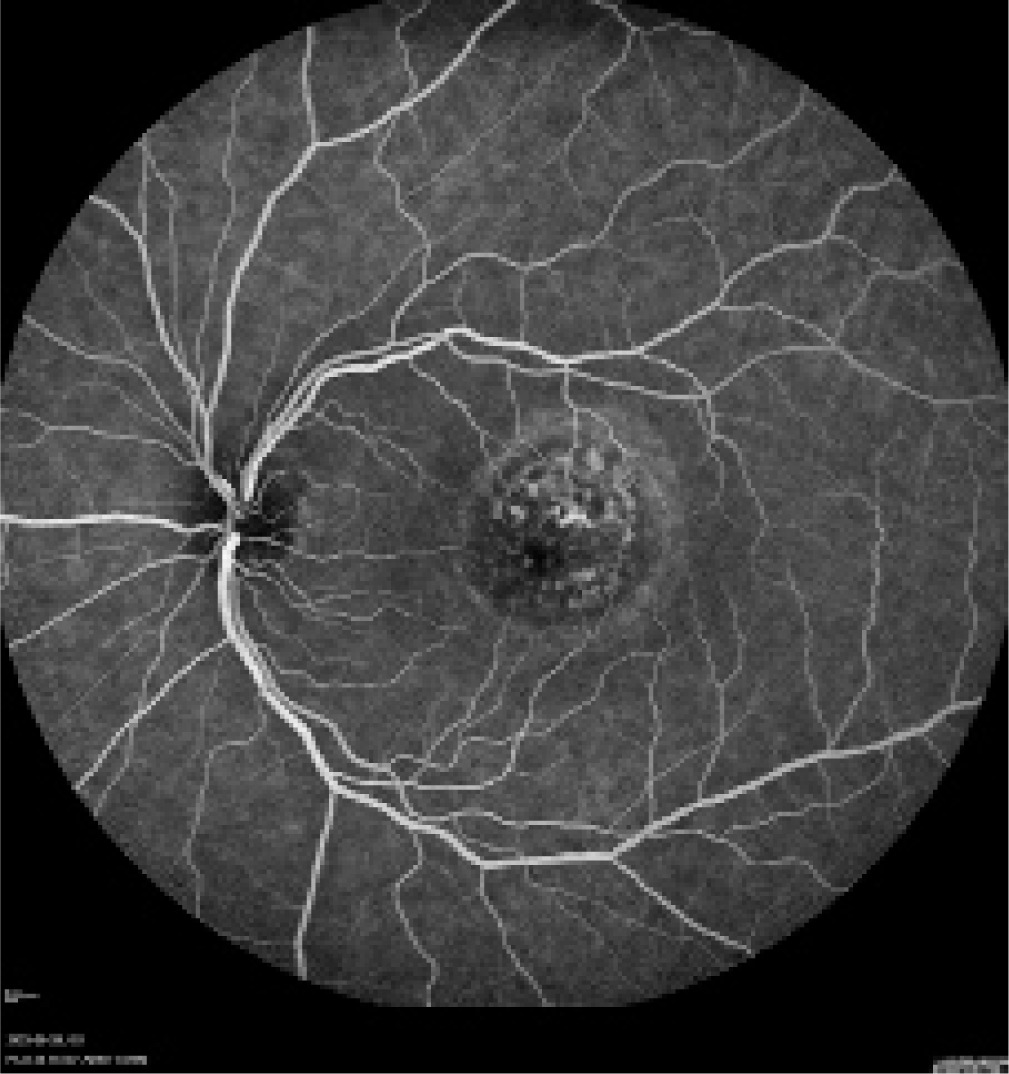
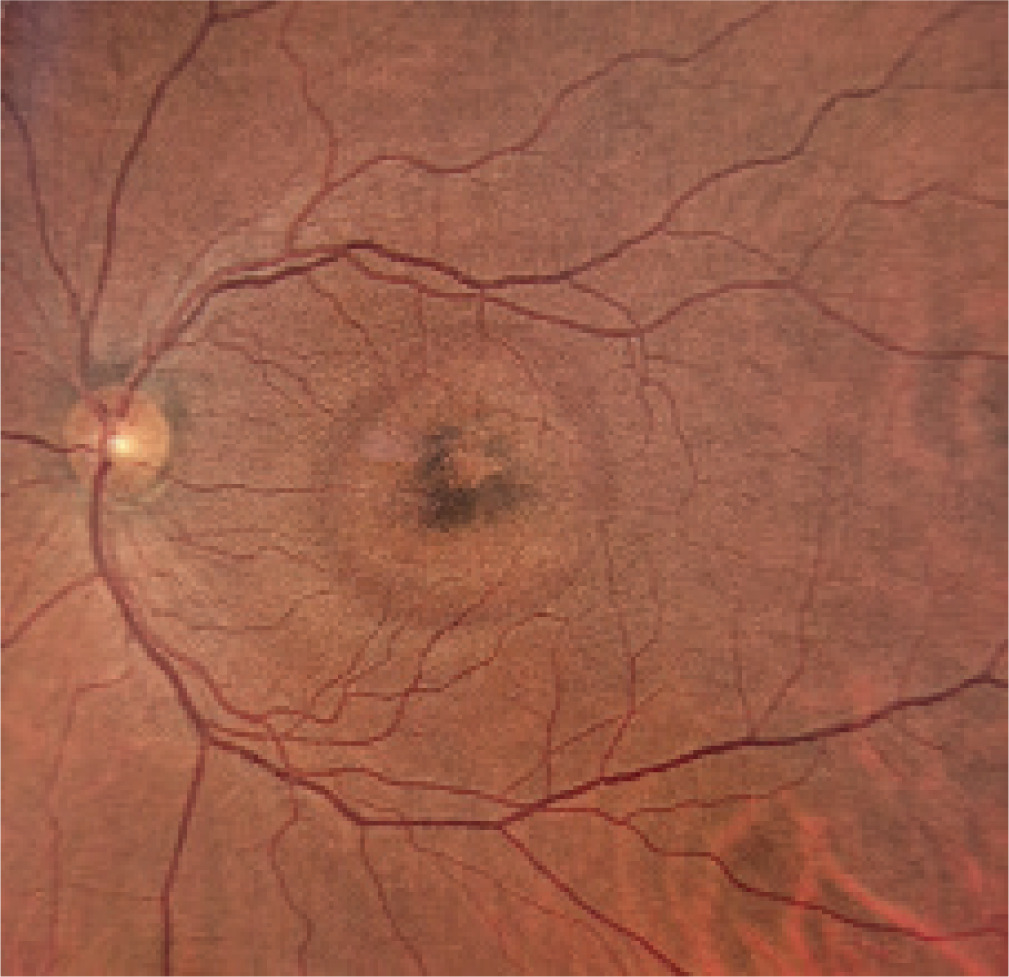
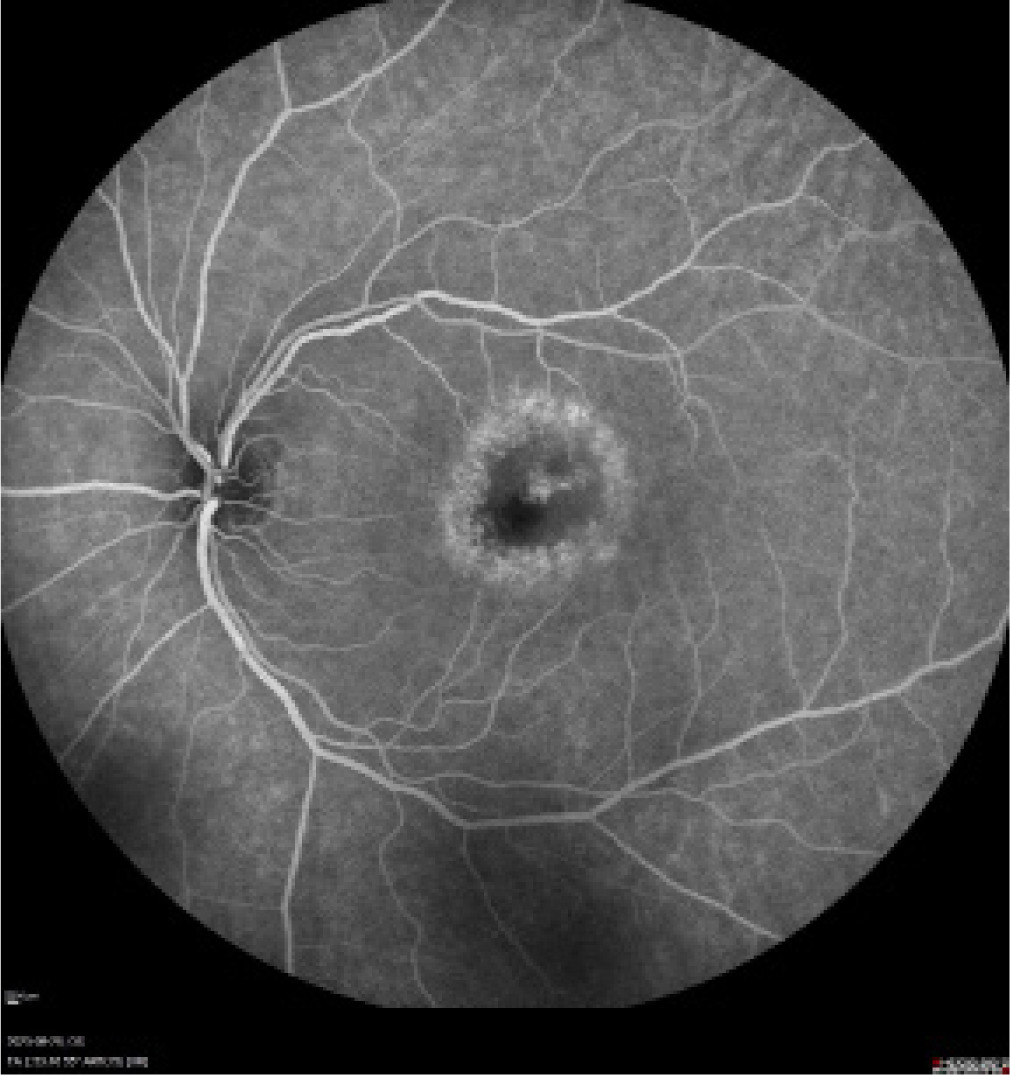
Diagnostic evaluations revealed findings consistent with retinal pathology, including changes observed in fluorescein angiography (FA) and OCT. Specifically, FA (Figure 1) displayed a halo of hyperfluorescence surrounding dark spots in the macular region. Figure 2 presents a color fundus photograph before initiation of treatment.
Figure 1
Left eye pretreatment fluorescein angiography – halo of hyperfluorescence surrounding dark spots in the macular region
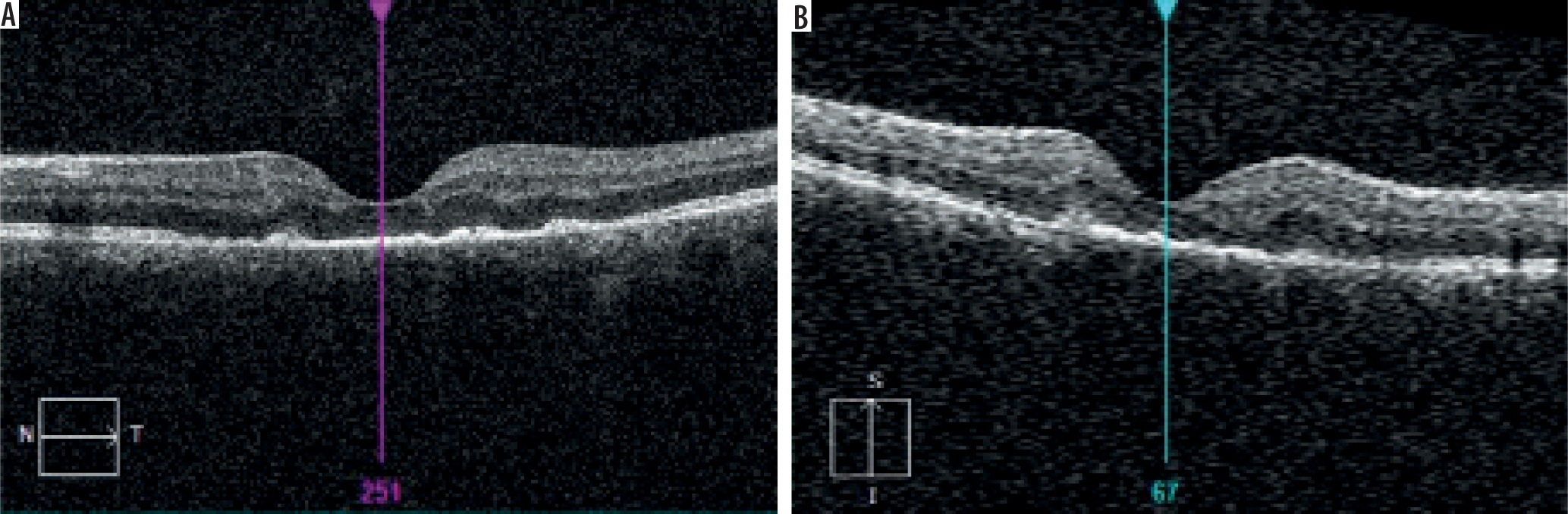
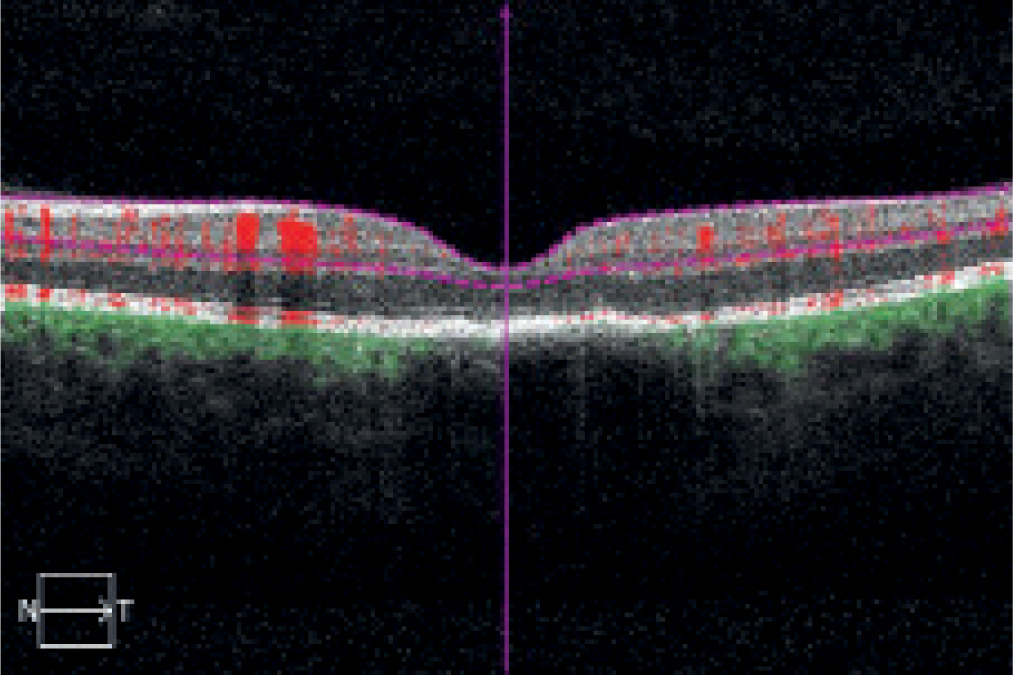
OCT demonstrated a malformed fovea centralis outline with discrete intraretinal edema, loss of photoreceptors, and hyperreflective deposits (Figure 3).
Figure 3
Optical coherence tomography with malformed fovea centralis outline with discrete intraretinal edema
Central serous chorioretinopathy (CSCR) was the initial diagnosis, and supportive therapy was initiated including dorzolamide 20 mg/ml 2 × 1, nepafenac 1 mg/ml 3 × 1, moisturizing eye drops 3 × 1, and a dietary supplement (lutein + zeaxanthin) 1 × 1.
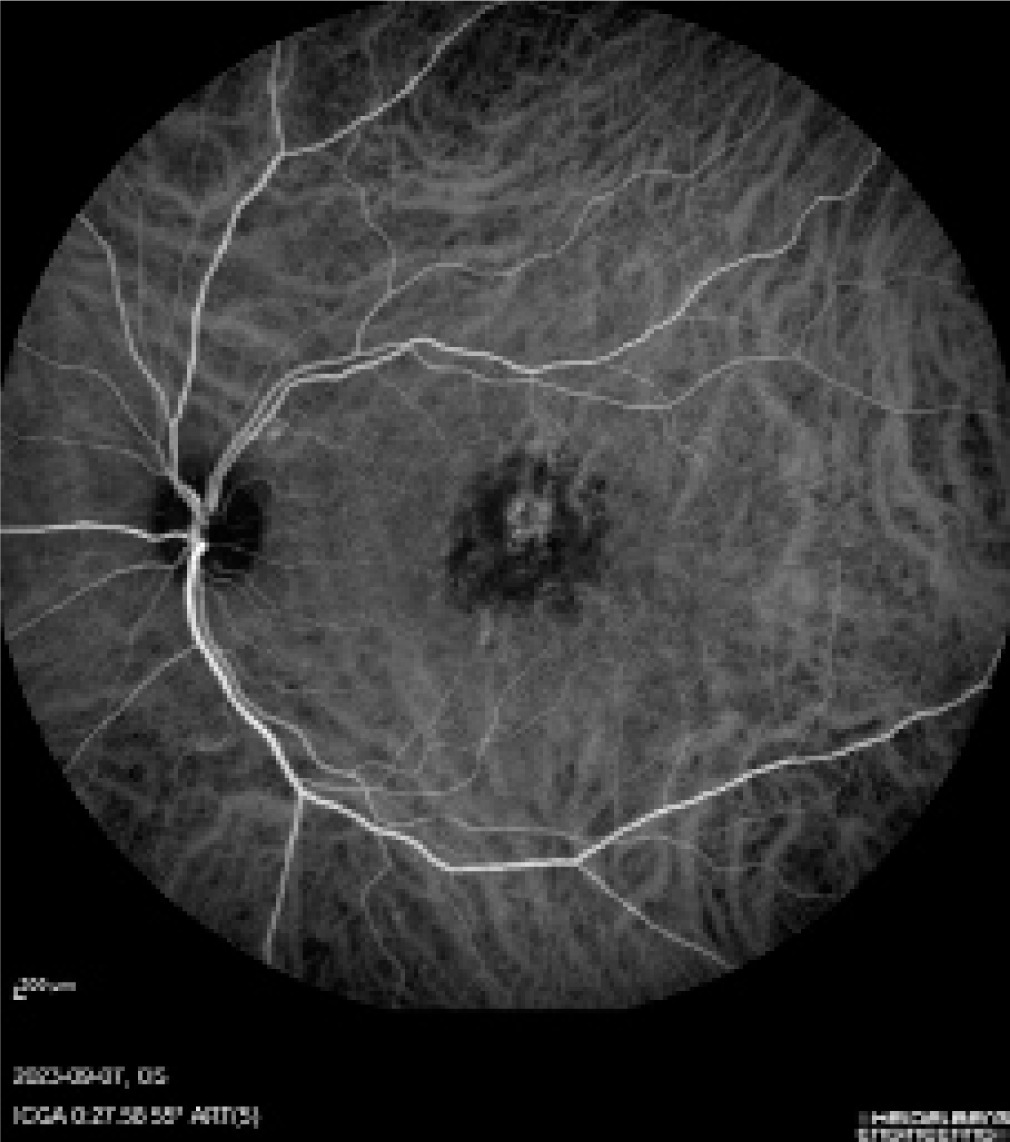
One week later, the patient returned to the emergency department with worsening vision (0.5/50) and new-onset dizziness, prompting admission to the ophthalmology department. During hospitalization, laboratory investigations revealed elevated levels of C-reactive protein and white blood cell count, neutrophils, D-dimer, and positive herpes simplex virus (HSV) IgM antibodies. A reassessment of the patient’s clinical presentation – considering the dynamic progression of findings, constellation of symptoms, and, most importantly, multimodal imaging – enabled the diagnosis of acute retinal pigment epitheliitis (ARPE). Figure 4 presents left eye indocyanine green angiography during treatment.
The patient received aggressive anti-inflammatory therapy, including oral acyclovir 800 mg 4 × 1, intravenous doxycycline 100 mg, intravenous methylprednisolone with tapering doses, and dalteparin 5000 IU. Topical treatment for the left eye comprised dorzolamide 20 mg/ml 2 × 1, diclofenac 1 mg/ml 2 × 1, and dexamethasone 1 mg/ml 2 × 1.
Hospitalization lasted one week, during which FA demonstrated treatment advancements and OCT revealed abnormalities in the pigment epithelial lineage with hyperreflective cavities under the neurosensory retina. Discharge from the hospital was accompanied by a left eye vision rating of 2/50 (Figure 5).
Post-discharge pharmacotherapy included continued acyclovir and oral methylprednisolone with tapering doses, along with topical pranoprofen 1 mg/ml 2 × 1 and loteprednol 5 mg/g 3 × 1 to the left eye.
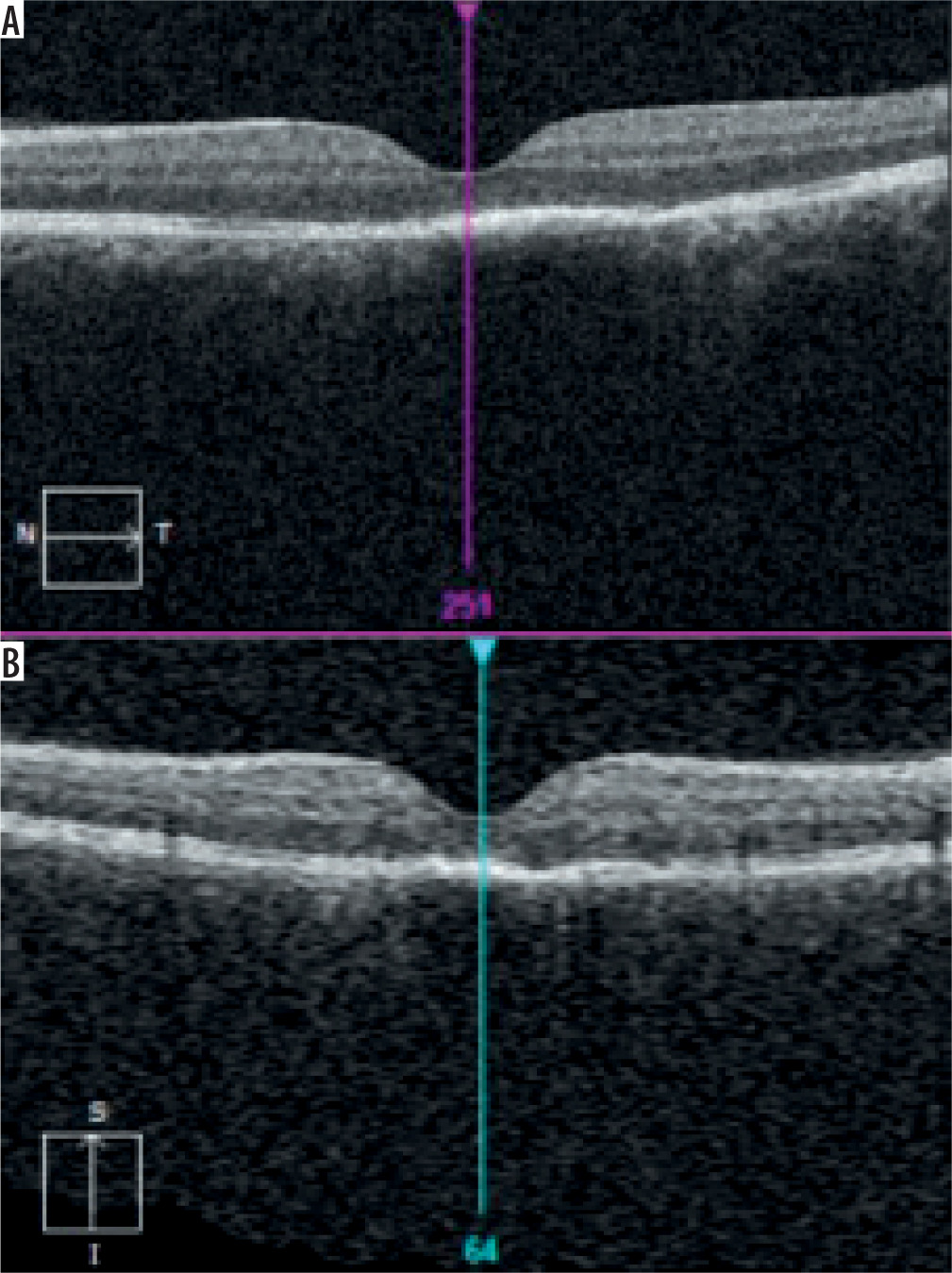
A follow-up visit after two weeks showed reduction of the lesion, with preserved foveal outline and evidence of retinal pigment epithelium (RPE) hyperplasia with photoreceptor loss. Left eye FA after 2 weeks of anti-inflammatory pharmacotherapy (Figure 6) showed a smaller, inactive lesion.
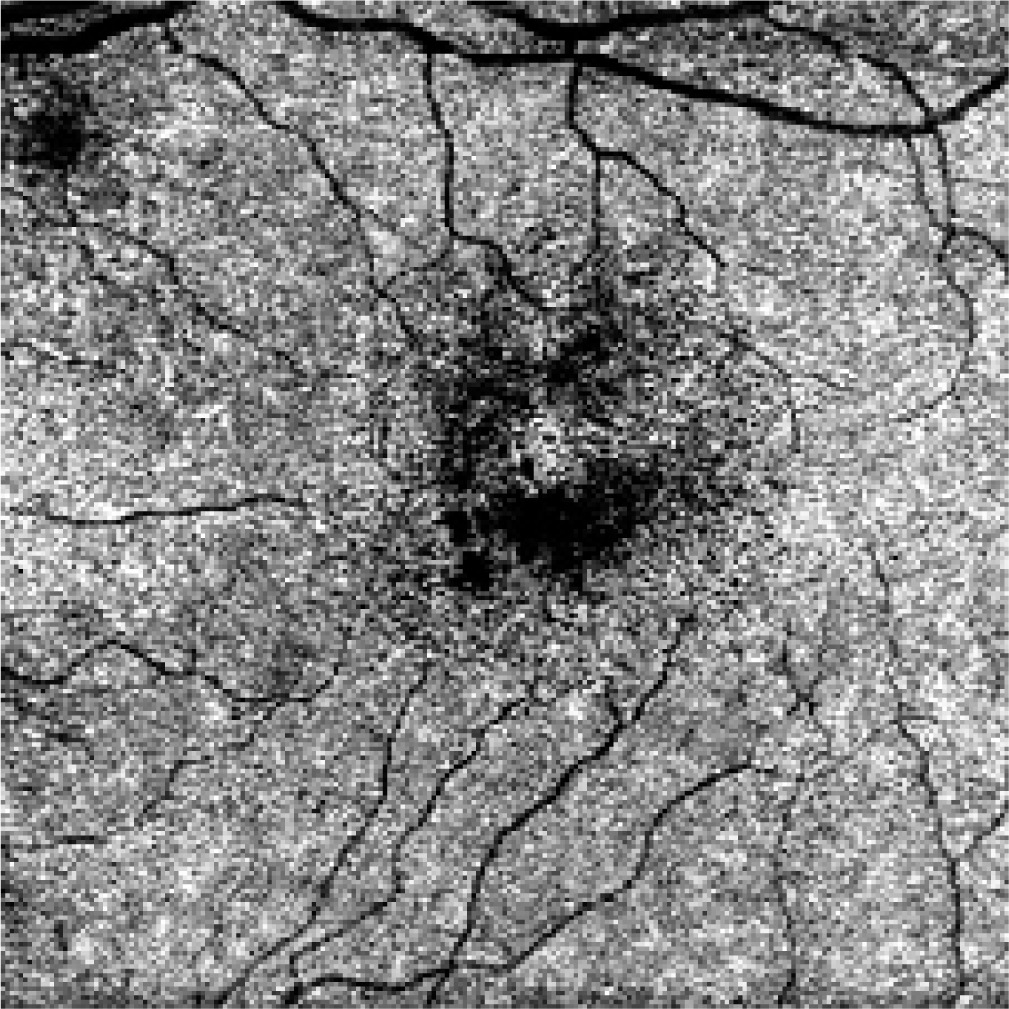
The RPE changes appeared as spots of hyperfluorescence in the macular area. At the one-month follow-up, visual acuity improved to 5/16. Multimodal imaging included post-treatment OCT (Figure 7) and OCT angiography (OCTA) imaging at the level of the choriocapillaris (Figure 8).
DISCUSSION
As Colucciello [8] noted, the etiology of ARPE remains incompletely understood; however, it is widely hypothesized to have an inflammatory origin, potentially provoked by viral infections or immune system dysregulation. Considering the patient’s clinical presentation, it is noteworthy that preceding the onset of ARPE, he exhibited flu-like symptoms, consistent with prodromal manifestations frequently reported in association with ARPE.
Additionally, ARPE’s potential to mimic other diseases underscores the necessity for meticulous differential diagnosis such as CSCR. When considering the differential diagnosis, it is also recommended to keep in mind vitelliform lesions of the central macula – such as adult foveomacular dystrophy and age-related macular degeneration – as well as white dot syndromes, including multiple evanescent white dot syndrome, acute macular neuroretinopathy, and acute posterior multifocal placoid pigment epitheliopathy [7]. These findings underscore the necessity of considering ARPE in the differential diagnosis of acute visual disturbances, particularly in younger individuals presenting with central scotomas [9].
In the present case, the initial CSCR supportive therapy was initiated, including dorzolamide, a topical carbonic anhydrase inhibitor which improves RPE fluid transport, promoting subretinal fluid resorption by enhancing ion flux across the RPE [10]. A multicenter randomized controlled trial demonstrated that lutein-based antioxidant supplementation in patients with chronic CSCR significantly improved best-corrected visual acuity and reduced subfoveal fluid height by 28.6% over six months, supporting its role in fluid resorption and disease modulation. Although our patient did not present with subretinal fluid, OCT revealed discrete intraretinal edema and RPE dysfunction. Based on lutein’s documented ability to support RPE function and modulate oxidative stress, its use in our case was aimed at enhancing the resolution of retinal fluid and stabilizing the retinal barrier. The rationale extends beyond CSCR and is supported by studies indicating that lutein may benefit various retinal pathologies involving oxidative stress and fluid imbalance, through its neuroprotective and anti-inflammatory properties [11].
ARPE is typically self-resolving, with symptoms subsiding spontaneously over a course of weeks to months. The visual prognosis is generally favorable, though infrequent recurrences have been documented. Management strategies are predominantly conservative, emphasizing regular monitoring and supportive interventions [7].
In the present case, the authors emphasize a multifaceted approach to preserve ocular function and prevent complications. Antiviral therapy, such as oral acyclovir and valacyclovir, plays a significant role in managing viral endotheliitis, often administered alongside corticosteroids to control inflammation and prevent rebound effects. In our patient, antiviral treatment with acyclovir was initiated due to active HSV infection confirmed by serological testing, which revealed positive HSV-specific IgM antibodies in the absence of IgG, indicating a primary or recent infection. Corticosteroids were used as an adjunct to reduce intraocular inflammation, a common response in viral retinal or endothelial infections. When used in combination with antiviral agents, corticosteroids can help prevent immune-mediated tissue damage while ensuring that viral replication is simultaneously suppressed, reducing the risk of exacerbating the infection. This dual therapeutic strategy is widely recommended in managing HSV-associated ocular inflammatory disorders, particularly when rapid control of inflammation is necessary to preserve visual function [12, 13]. In order to avoid secondary bacterial infection, anti-biotic therapy, such as doxycycline, provides necessary coverage [14]. Given the potential for vascular complications, anticoagulants such as low molecular weight heparins help to minimize the risk of thrombosis [15]. Furthermore, topical treatment with dexamethasone reduces inflammation and stabilizes endothelial function [16], diclofenac provides additional anti-inflammatory support while minimizing steroid-related internal ocular pressure risk, and carbonic anhydrase inhibitors ensure internal ocular pressure control, preventing glaucomatous damage. Together, these treatments address the diverse pathological mechanisms of ARPE, improving patient outcomes and reducing the risk of long-term visual impairment.
Thomas [17] emphasized that state-of-the-art technologies, including spectral-domain OCT and OCTA, have greatly improved the accuracy of early diagnosis. These imaging techniques frequently reveal distinctive hyper-reflective abnormalities at the level of the retinal pigment epithelium, often accompanied by disruption of the photo-receptor layer. Additionally, multicolor imaging has emerged as a valuable adjunctive diagnostic approach. Early changes can be observed both in FA (as a halo of hyperfluorescence in the early phase surrounding the dark spots seen ophthalmoscopically in the macular region) and in OCT. During the hospital admission, fluorescein angiography revealed progressive improvement in response to treatment, while OCT demonstrated distinct hyperreflective alterations predominantly affecting the outer retinal layers, particularly the photoreceptor segments and the RPE. These manifestations are characterized by hyperreflective foci localized within the ellipsoid zone (EZ), frequently extending into the interdigitation zone (IZ). In certain cases, disruption of the external limiting membrane is evident, accompanied by varying degrees of outer nuclear layer involvement. During the acute phase, localized hyperreflectivity within the outer retina is a hallmark feature, which typically diminishes over time, occasionally resulting in persistent irregularities of the IZ and EZ. Following two weeks of pharmacological intervention, FA indicated a reduction in lesion size and activity, accompanied by areas of hyperfluorescence in the macular region, suggestive of retinal pigment epithelium alterations. Concurrent OCT imaging showed preservation of the foveal contour, RPE hyperplasia, and photoreceptor loss. These findings underscore the critical roles of both OCT and FA in the precise diagnosis and management of inflammatory retinal disorders. The complementary use of these imaging modalities enables detailed visualization of structural and functional changes, facilitating more accurate treatment strategies.
All the mentioned factors collectively contribute to a comprehensive understanding of the patient’s case, underscoring the imperative of integrating clinical and epidemiological elements in the diagnosis and management of ARPE.
In summary, the unconventional course of ARPE observed in this case highlights the inherent variability in disease presentation and treatment response. This underscores the necessity for a holistic approach, synthesizing diverse clinical and epidemiological factors, to effectively navigate and manage ARPE cases.







