
INTRODUCTION
Functional vision – defined as the ability to move independently, navigate spatial environments, and perform sight-dependent daily tasks – is a key determinant of quality of life [1]. In individuals with low vision, spatial orientation relies more heavily on contrast sensitivity and visual field than on visual acuity alone. Accurate assessment of functional vision is therefore crucial, particularly in patients with rare genetic retinal conditions, such as those related to RPE65 gene mutations, who may be eligible for gene therapy [2].
Mutations in the RPE65 gene lead to inherited retinal dystrophies characterized by progressive vision loss [3, 4]. The RPE65 gene encodes the RPE65 protein (an isomerohydrolase), a key enzyme in the retinoid cycle responsible for the conversion of all-trans-retinyl to 11-cis-retinal. This isomer is essential for the regeneration of rhodopsin, the light-sensitive pigment responsible for vision under low-light (scotopic) conditions [5]. RPE65 mutations lead to the accumulation of toxic by-products of the visual cycle, impairing the ability of retinal pigment epithelial (RPE) cells to respond to light stimuli. Consequently, progressive degeneration of RPE cells occurs, followed by photoreceptor degeneration, leading to significant vision deterioration. Diseases potentially caused by RPE65 mutations include, among others, Leber congenital amaurosis (LCA) and retinitis pigmentosa (RP) [6]. Mutations in the RPE65 gene are inherited in an autosomal recessive manner, meaning that symptoms occur in individuals who carry two mutated copies of the gene. They lead to progressive retinal degeneration, typically presenting as night blindness, reduced visual acuity, and narrowing of the visual field. Most individuals affected by RPE65 mutations meet U.S. criteria for legal blindness before the age of 18.
A major milestone in the treatment of patients with biallelic RPE65 mutations was achieved in 2017, when the U.S. Food and Drug Administration (FDA) approved the first gene therapy – voretigene neparvovec (Luxturna) [3]. In Europe, the therapy was approved by the European Medicines Agency (EMA) at the end of 2018. The first administration of voretigene neparvovec in Poland was carried out by our team in 2021 at the Eye Diseases Clinic, Poznań University of Medical Sciences. The therapy involves delivering a functional copy of the RPE65 gene into RPE cells using an AAV2 viral vector. The aim of treatment is to restore retinoid cycle function, thereby enhancing vision or at least slowing the progression of vision loss.
An objective measurement of improvement in functional vision is crucial for evaluating the effectiveness of gene therapy [7]. To this end, the MLMT (Multi-Luminance Mobility Test) was developed – a standardized tool used to assess a patient’s ability to navigate under controlled lighting conditions (Table I), simulating various real-life situations [2]. The MLMT is a test combining research and clinical elements to replicate the challenges associated with everyday mobility under controlled conditions [3]. The MLMT results are among the primary criteria for evaluating the efficacy of voretigene neparvovec therapy.
Table I
Light intensity levels and corresponding real-world conditions
The aim of this study is to present and analyze in detail the MLMT results in a group of four patients with confirmed biallelic RPE65 gene mutations who underwent gene therapy with voretigene neparvovec (Luxturna). The test protocol and its significance in assessing patients’ functional vision before and after treatment are discussed. Presenting these clinical outcomes contributes to a better understanding of the impact of gene therapy on functional vision and its potential to improve the quality of life in individuals affected by these conditions.
MATERIAL AND METHODS
Patients with confirmed biallelic RPE65 gene mutations were assessed using the MLMT before and at 30 and 90 days after the administration of subretinal gene therapy with voretigene neparvovec (Luxturna). The test aimed to objectively measure changes in functional vision under controlled lighting conditions [2].
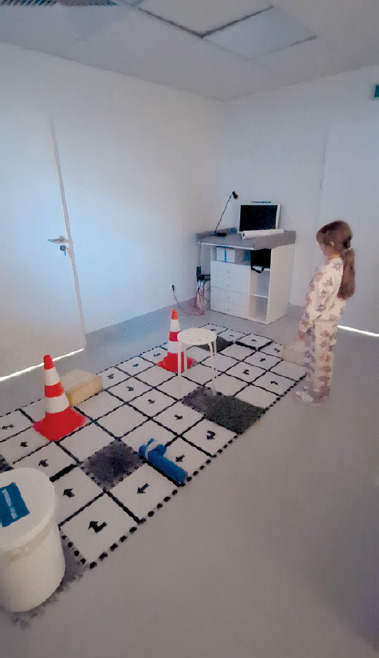
The detailed methodology for test setup and evaluation was described by Chung et al. [2]. During the test, participants were required to complete a standardized obstacle course (Figure 1). To minimize the learning effect, the course configuration was modified after each run. Twelve unique MLMT course configurations were available. Each path was visually marked with black arrows, scaled to correspond to a visual acuity of 0.1 at a distance of 2 m on a Snellen chart. The course itself consisted of 50 white, square tiles measuring 30 × 30 cm, of which 24 tiles had printed arrows indicating the direction. The topology of the course, including the number of turns and types of obstacles, was standardized. Additionally, 15 obstacles were positioned along the course, including two raised steps with directional markings, two tiles covered with artificial grass, two elevated polyurethane foam blocks, two Styrofoam cones, three black tiles representing holes in the ground, a single step-over obstacle, a standing fan, a STOP road sign, and a trash can.
Before performing the test, patients were dark-adapted for a period of 40 minutes. The MLMT was conducted at seven progressively increasing illumination levels, ranging from 1 lux to 400 lux. The lowest illumination level at which the patient successfully completed the course was recorded, along with one level below and one or two levels above this threshold. The range was selected to reflect real-world lighting conditions – from dim night-time illumination to bright indoor lighting – enabling a comprehensive assessment of functional vision across varied environmental scenarios.
Multi-Luminance Mobility Test scoring included the following parameters: total course completion time and the number of errors. Navigation accuracy was quantified as the percentage of errors, calculated by dividing the number of collisions with obstacles by the total number of obstacles on the course. Total completion time consisted of the actual time taken to finish the course plus time penalties for specific infractions: deviation from the designated path (+15 seconds), skipping tiles marking the route (+15 seconds per missed tile), and the need for verbal intervention from the examiner to redirect the patient (+30 seconds per intervention). The passing criterion for the MLMT at a given light level was completing the course within 180 seconds and making no more than three errors.
RESULTS
Four patients with RPE65 mutations – two diagnosed with LCA (P1, P4) and two with RP (P2, P3) – underwent the MLMT. Following ophthalmological assessment, the patients received a subretinal injection of Luxturna in one eye.
Prior to gene therapy, patient P1 was unable to pass the test at any of the evaluated lighting levels, showing difficulty in perceiving visual stimuli even at 400 lux, both during monocular testing (left eye, before treatment) and binocular testing. Patient P2 passed the test at 4 lux in monocular testing (right eye before the administration of therapy) and at 1 lux in binocular testing. Before therapy, patient P3 completed the test at 1 lux under both monocular (right eye, pre-treatment) and binocular conditions; however, due to low accuracy, he did not pass the monocular test. The final patient analyzed, P4, completed the test at 50 lux under both monocular conditions (right eye, before therapy) and binocular conditions. However, similar to patient P3, more than three errors were made during the monocular test, resulting in a passing score only at 250 lux under monocular conditions. Detailed MLMT results prior to Luxturna administration are listed in Table II.
Table II
MLMT results before therapy administration
One month after receiving Luxturna, patient P1 showed improvement, passing the test at 400 lux with the treated (left) eye as well as under binocular conditions. However, lower illumination levels still posed a challenge. Patient P2 reduced test completion time at most lighting levels. He successfully completed all levels except 1 lux with the treated (right) eye, where he did not meet the required accuracy threshold. Patient P3 maintained the ability to pass the test at all illumination levels in the monocular test (right eye after treatment) and binocular test. An improvement in accuracy and a reduction in test completion time were noted. Patient P4 passed the test at an illumination level of 1 lux in the monocular test (right eye after treatment) and in the binocular test. However, due to low accuracy, the monocular test was only considered passed at 4 lux in the monocular setting (right eye after gene therapy). Table III presents detailed data on the patients’ ability to pass the MLMT depending on illumination level, 30 days after the administration of Luxturna.
Table III
MLMT results at 30 days after therapy administration
Three months after receiving gene therapy, patient P1 successfully completed the test at an illumination level of 50 lux using the treated (left) eye. Due to low accuracy, the test was considered passed at 400 lux for the left eye and at 250 and 400 lux in the binocular assessment. At higher illumination levels, the patient made fewer errors, although the time required to complete the test increased. Patient P2 showed a decline in visual performance in both the treated (right) eye and binocular assessments, in terms of both accuracy and completion time, compared to previous visits. He was still unable to pass the test at 1 lux with the treated (right) eye, as he did not meet the accuracy and final time criteria. Patient P3 demonstrated continued improvement, with increased accuracy and reduced test completion time during both right-eye and binocular assessments. He achieved the best results in the study group. Patient P4 demonstrated improvement relative to previous visits, successfully completing the test at 1 lux with the right eye. At the remaining illumination levels, the test completion time decreased and the number of errors was reduced, which improved his accuracy. Table IV presents detailed data on the patients’ ability to pass the MLMT depending on illumination level, 90 days after the administration of Luxturna.
Table IV
MLMT results at 90 days after therapy administration
The overall analysis of MLMT results demonstrates a clear improvement in patients’ navigational abilities following gene therapy. After 90 days, patient P1, who was unable to pass any level of the test before treatment, was able to complete the test at 400 lux (left eye) and at 250 and 400 lux (binocularly) after therapy. Patient P2 did not show significant improvement – he continued to pass the test at 4 lux (right eye) and 1 lux (binocularly). Patient P3, who was already able to pass the test at the 1 lux level before therapy, continued to achieve the best results in the group, showing improvement in both accuracy and test completion time. Patient P4 was able to pass the test at an illumination level of 250 lux (monocular test prior to gene therapy) and 50 lux (binocular test). Three months after gene therapy administration, P4 was able to complete the test at an illumination level of 1 lux under monocular conditions (right eye after gene therapy) as well as under binocular conditions. Therefore, it can be concluded that the MLMT level improvement was 5 levels for the monocular test (right eye after gene therapy) and 3 levels for the binocular test.
DISCUSSION
The MLMT is an objective method for evaluating functional vision by assessing a patient’s ability to navigate a standardized obstacle course under variable lighting conditions [2]. The passing criteria, which include completing the test in under 180 seconds and achieving an accuracy threshold, reflect both the speed of visual information processing and the precision of movements in response to visual stimuli. Prior to the administration of Luxturna gene therapy, the patients with confirmed RPE65 gene mutations demonstrated significant difficulty completing the MLMT, particularly under lower light conditions. This deficit, particularly evident under conditions simulating low-light environments, is consistent with the impaired dark adaptation and night vision typically associated with this genetically determined retinal dystrophy [8].
Following a single administration of Luxturna, a consistent improvement in MLMT performance was observed in three of the four patients analyzed, while the fourth showed stabilization. This favorable change was reflected in a reduction in the number of errors made, a shorter total course completion time, and an overall improvement in navigation accuracy. Notably, the most significant improvement was observed in navigation under low-light conditions, suggesting that gene therapy contributed effectively to the restoration of photoreceptor function responsible for vision in such environments [4]. Additionally, a correlation was observed between baseline best-corrected visual acuity (BCVA) and MLMT results after therapy. Patients who had relatively better visual acuity before the intervention achieved higher MLMT scores. Due to the limited sample size, statistical analysis of this observation was not possible. Detailed visual acuity results for this Polish patient cohort were published by our team separately in Klinika Oczna [Acta Ophthalmologica Polonica].
Our findings suggest that the MLMT serves as a valuable and sensitive tool for assessing the natural progression of inherited retinal diseases [3], as well as for monitoring the therapeutic efficacy of gene therapies such as Luxturna [9]. Unlike static visual acuity tests, the MLMT enables a comprehensive evaluation of functional vision under near-real-life conditions, taking into account the dynamic aspects of visual perception under varying lighting conditions. This makes it particularly valuable for assessing the impact of therapy on patients’ capacity to perform everyday activities [10].
It should be noted that the management of patients with retinal dystrophy is a multifaceted process that extends beyond the monitoring of objective visual parameters. In addition to regular monitoring of disease progression, patient and family education plays a key role in understanding the nature of the condition, potential therapeutic options, and adaptive strategies. Vision rehabilitation, which focuses on maximizing the use of remaining visual function, plays a key role in enhancing patients’ quality of life [11]. In cases of significant visual impairment, low vision aids can be invaluable, including magnifying lenses, image enlargement systems, electronic reading devices, and specially adapted everyday items that facilitate the performance of routine activities.
The results of this study, although based on a small group of four patients, are consistent with observations from larger clinical trials confirming the effectiveness of Luxturna in improving functional vision in individuals with RPE65 gene mutations [3]. Notably, the improvement observed in the MLMT extended beyond quantitative measures (e.g. completion time) to include qualitative aspects such as increased movement confidence and reduced hesitation during navigation, as evidenced through video analysis. It can be speculated that this improvement results from the restoration of the retinoid cycle in the retina, which directly enhances photoreceptor sensitivity to light, especially under low illumination [13].
In the context of current knowledge, traditional assessment methods, such as visual acuity testing, may not fully reflect the actual improvement in functional vision following gene therapy. Due to its dynamic structure and incorporation of varying illumination levels, the MLMT appears to be a more sensitive measure for detecting subtle changes in visual function under conditions that closely resemble real life [2]. This supports its potential utility as an important tool for assessing the effects of treatment for retinal dystrophy.
However, certain limitations of the MLMT should also be acknowledged. While efforts were made to minimize the impact of learning effects through appropriate testing protocols, their influence – particularly during repeated assessments – cannot be entirely excluded. Furthermore, in patients demonstrating marked improvements in vision, the MLMT may exhibit a ‘ceiling effect’ where further enhancements in functional vision are no longer reflected by any significant changes in test results. Consequently, MLMT outcomes should always be interpreted within the context of a comprehensive evaluation of the patient’s condition, including subjective reports and everyday visual functioning.
CONCLUSIONS
Future studies involving larger patient cohorts will help to more precisely establish the minimal clinically important difference (MCID) in MLMT performance, thereby facilitating interpretation of changes following therapeutic intervention. Comparing the results of the MLMT with the results of other tests assessing functional vision, such as mobility tests conducted in real-world settings [13], could provide additional valuable insights into the utility of the MLMT.
In conclusion, although limited by a small patient group, this clinical report supports the use of the MLMT as an effective tool for monitoring the outcomes of Luxturna gene therapy in individuals with RPE65 mutations. The observed improvements in MLMT performance, especially under low-light conditions, indicate a meaningful therapeutic benefit that extends beyond changes in visual acuity alone. Integrating the MLMT into the comprehensive care of patients with retinal dystrophies may contribute to a better understanding of the impact of therapeutic interventions on quality of life.







