
INTRODUCTION
Erysipelas is an acute inflammation of the skin and subcutaneous tissue, most commonly caused by group A streptococci, and occasionally by group C and G streptococci, or other pathogens. It typically develops after bacterial inoculation through a disruption in the protective barrier of the skin or mucous membranes. The etiology may be odontogenic, post-traumatic, related to sinus pathology, skin infections, or idiopathic in nature [1-4]. It is characterized by severe local erythema, swelling, shiny skin, warmth, and tenderness upon palpation, with clear demarcation between the affected area and healthy tissues. Inflammation spreads rapidly through the lymphatic system. The condition can affect individuals of all age groups, and the most common sites are the lower limbs and face, which accounts for as much as 4-24% of cases [5, 6]. Erysipelas may be accompanied by systemic symptoms induced by exotoxins, including flu-like symptoms, chills, fever, and vomiting. Complications may include abscess formation, necrotizing fasciitis, sepsis, recurrent infections, and lymphedema [7].
The differential diagnosis should consider insect bites and stings, pyoderma gangrenosum, herpetic infections, contact dermatitis, and paraneoplastic syndrome (carcinoma erysipeloides) [8].
In most cases, both local and systemic conservative treatments yield positive therapeutic outcomes. In severe and complicated cases, surgical intervention is required, including debridement of necrotic tissues, drainage of abscesses, and decompression of affected anatomical spaces [9].
The study group included adults aged 39 to 69. The patients were evaluated based on ophthalmic and systemic symptoms, inflammatory markers, microbiological test results, treatment methods administered, and the final therapeutic outcome.
The aim of the study is to raise clinicians’ awareness of facial soft tissue infection, thereby minimizing the risk of complications and preventing the neglect of symptoms of developing erysipelas, which can lead to permanent health damage or even death.
Clinical information
The clinical data are presented in Table I.
Table I
Clinical information
Description of selected cases
Case report 1
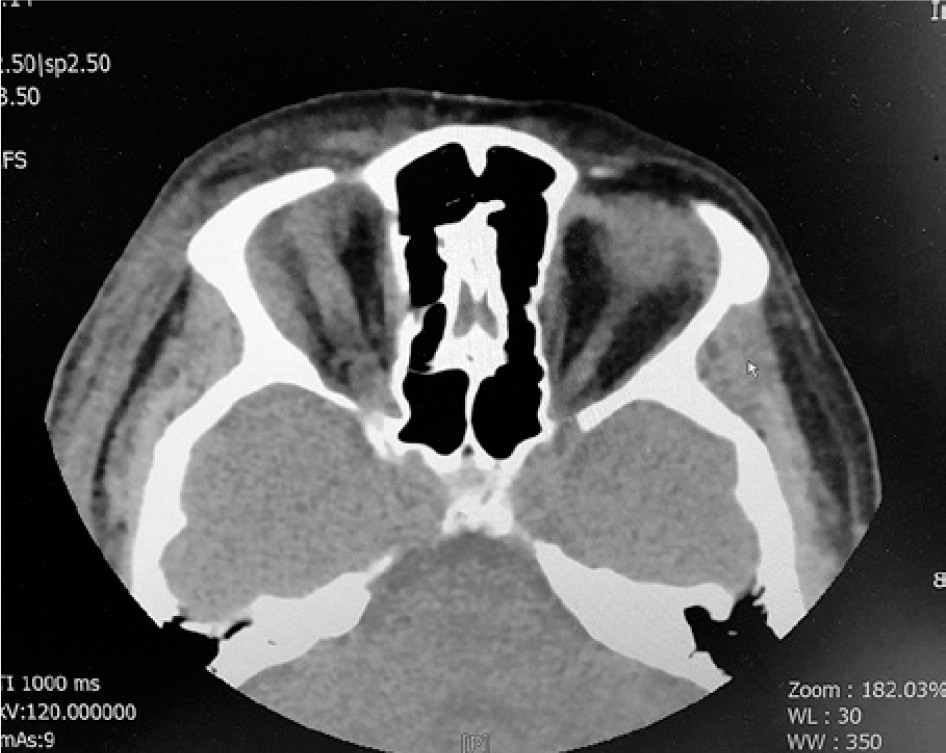
A 39-year-old female patient presented to the hospital emergency department with significant swelling of the right eyelid and erythema on the right side of her face, which had been progressively worsening over several hours. Due to the severity of the inflammation, the palpebral fissure was closed, preventing mechanical opening and assessment of visual acuity. Laboratory markers of inflammation, except for procalcitonin, were significantly elevated, accompanied by a high fever. A few days prior, the patient had sustained damage to the right nasal mucosa, and on the day of admission, a 0.5 cm blister filled with serous fluid was noted on the right upper eyelid. Contrast-enhanced computed tomography (CT) revealed severe inflammation of the preseptal connective tissue. Suspicions arose that the inflammatory changes were altering the shape of the anterior chamber of the right eye, with possible infiltration of the anterior ocular segment. The patient was admitted for systemic treatment, and empirical antibiotic therapy was started within the first 24 hours. A conjunctival swab from the right eye confirmed a streptococcal etiology of the infection, while blood cultures showed no pathogens. During the first two days of treatment, a significant increase in inflammatory markers was observed, with peak values of CRP at 347 mg/dl, procalcitonin at 5.73 ng/ml, and leukocytosis at 18.57 G/l. Anticoagulation treatment was implemented. By the third day of therapy, a positive clinical response to treatment was observed. However, significant edema persisted over the following days, accompanied by a progressive necrotic process affecting the eyelids of the right eye. On the seventh day of hospitalization, necrotic tissue was surgically removed (Figures 1, 2). Intraoperatively, a deep infiltration involving the orbicularis oculi and levator palpebrae superioris muscles of the right eye was identified. An ophthalmological examination of the anterior segment of the right eye showed no evidence of inflammatory infiltration or post-traumatic changes. To accelerate the healing process of the postoperative site, a decision was made to initiate hyperbaric oxygen therapy, consisting of 12 sessions. Following three weeks of intensive hospital treatment, the patient was discharged home with fully restored visual acuity and marked improvement in both her local symptoms and overall condition. Due to the extensive tissue necrosis, ptosis persisted after complete wound healing, along with partial fibrosis of the eyelids, but without symblepharon or signs of lagophthalmos.


Case report 2
A 51-year-old female patient presented to the Emergency Department in Zadar, Croatia, where she was vacationing, with worsening edema and phlegmon in the soft tissues of the right eyelids, periorbital region, and cheek. Three days earlier, the patient sustained an injury to the right side of the face with a metal rod, resulting in a skin wound in the right orbital region. Radiographic examinations ruled out fractures of the facial bones. Laboratory tests showed elevated inflammatory markers, with a CRP level of 498.0 mg/l.
The patient was admitted to the Otolaryngology Department of the local hospital, where on the same day a procedure was performed to debride necrotic tissue from the upper eyelid. Additionally, a supraorbital and preauricular incision was made, and drainage was inserted. A swab taken during the procedure revealed the presence of Streptococcus pyogenes in the wound. Systemic antibiotic therapy was initiated with amoxicillin/clavulanic acid and clindamycin.
During her hospitalization, the patient received an ophthalmological consultation. According to the medical documentation, visual acuity was preliminarily assessed as normal after opening the palpebral fissure. Further conservative treatment and magnetic resonance imaging of the orbits were recommended. After five days of hospitalization, the patient’s condition gradually improved. However, despite the recommendation for continued hospital treatment, she discharged herself at her own request to travel back to Poland.
After returning to Poland, the patient was hospitalized at St. Adalbert’s Hospital in Gdansk. Along with persistent inflammation of the facial skin (Figure 3), she reported a deterioration in vision in her right eye. Ophthalmological examination revealed that the visual acuity in the right eye was limited to light perception, with accurate localization across all quadrants. Following an otolaryngology consultation, the decision was made to continue the treatment in the Otolaryngology Department.

Magnetic resonance imaging (MRI) of the orbits revealed inflammatory infiltration of the adipose and subcutaneous tissues of the right orbit, extending to the lacrimal gland, superior and lateral rectus muscles, and partially involving the right ethmoid. Additionally, pathological post-contrast enhancement of the right optic nerve was observed, extending over a 10 mm segment in the intraorbital region, consistent with neuritis (Figure 4).
The patient underwent endoscopic right orbital decompression and a right lateral craniotomy. Necrotic tissue was again removed from the eyelid wound. Conservative treatment with antibiotics was continued, and hyperbaric therapy was initiated. After achieving improvement of the local condition, upper eyelid blepharoplasty was performed using a split-thickness flap taken from the thigh, resulting in complete wound closure. During a follow-up ophthalmological consultation, absence of light perception was noted in the right eye. The right optic disc appeared pale with blurred boundaries. The upper eyelid was drooping, with levator muscle activity limited to approximately 5 mm. The visual function of the right eye has been permanently lost.
Discussion
The cases analyzed above represent a broad spectrum of severity in S. pyogenes infections.
In one of the five patients, the infection course was relatively mild and could be effectively managed with systemic antibiotic therapy. The remaining 80% of patients developed necrotizing fasciitis, requiring additional surgical debridement. In one of the five reported cases, the infection extended to the intraorbital tissues, resulting in permanent and complete vision loss. Moreover, one patient developed sepsis as a complication of the infection.
Erysipelas is a skin inflammation most commonly caused by S. pyogenes bacteria.
Approximately 9% of erysipelas cases affect the facial area, which may require an ophthalmological consultation. Local signs of infection include a well-defined, red inflammatory infiltrate accompanied by localized edema. Furthermore, patients may report symptoms such as nausea, pain, and fever [10].
Streptococcus pyogenes is the most common pathogen responsible for necrotizing fasciitis, both as a sole agent and in mixed etiology infections [13]. Erysipelas and the associated necrotizing fasciitis are differentiated based on their clinical features. In the inflamed tissues, thrombosis of small vessels occurs, resulting in ischemia and necrosis. Signs indicating deeper structure involvement include blister formation within the affected area, intense pain or loss of sensation, epidermal sloughing, and visible necrotic regions [11, 12].
Accurate diagnosis is critical to ensure the timely initiation of appropriate therapy. In cases of erysipelas, immediate systemic antibiotic treatment should be administered without delay. If the clinical presentation indicates necrotizing inflammation of deeper tissues, urgent surgical intervention − involving the resection of necrotic tissues – should be performed alongside conservative treatment. This approach is essential to halt the progression of infection and establish optimal conditions for healing. The procedure should target only necrotic tissue, preserving as much skin, muscle, nerve, and vascular tissue as possible to ensure the best functional outcome [13]. In severe cases where orbital tissues are extensively affected, exenteration may be required to prevent the infection from spreading to the central nervous system (CNS) [13].
Necrotizing fasciitis is linked to several risk factors, including diabetes, hypertension, chronic alcohol abuse, and immunosuppression. However, nearly half of the patients have no underlying conditions that could predispose them to infection [13, 14]. Among the patients analyzed in this study, 80% had no underlying internal medicine conditions. In one case (20%), diabetes was diagnosed.
Without prompt treatment, patients may develop multiple organ failure or septic shock, potentially leading to death. CT or MRI can be used to evaluate the spread of the infection, while microbiological analysis of wound swabs aids in determining the appropriate antibiotic treatment.
The mortality rate for facial necrotizing fasciitis is lower than in other regions, with reports indicating a rate of 12.3%. Risk factors that increase mortality include patient age and the presence of diabetes [13]. The most critical factor associated with patient death is the lack of or delayed surgical debridement of the wound [15].
Conclusions
Bacterial infection of the periorbital tissues caused by S. pyogenes is a rare but highly dangerous condition that can result in a range of severe clinical complications, as highlighted above. Therapeutic success largely hinges on prompt diagnosis and timely surgical intervention in complex cases. Therefore, it is crucial to enhance education and raise awareness among healthcare professionals about the early signs of a developing infection.







