
INTRODUCTION
Vitrectomy is a microsurgical procedure that has been effectively performed since 1978 [1]. It is used in the treatment of retinal diseases [2]. One of the increasingly common steps in this procedure is the removal of the internal limiting membrane (ILM) [3]. The ILM is a critical anatomical and functional component of the retina. It serves as a barrier between the vitreous body and the retinal cell layers, playing a role in maintaining the structural and functional integrity of the retina.
The purpose of this article is to provide an in-depth analysis of the role of ILM peeling in vitreoretinal surgery. It focuses on the latest advancements in indications and surgical techniques, aiming to offer a detailed examination of the associated benefits and potential complications of ILM peeling.
The ILM is composed of Müller cells and a basement membrane, which includes collagen fibers, glycosaminoglycans, laminins, and fibronectin. The elements of the basement membrane are connected by peripheral fibers of the cortical part of the vitreous body [4]. The thickness of the ILM varies in different areas of the retina, being thicker over the macula and gradually thinning toward the periphery [5].
The ILM thickens and assumes a conical shape in the center of the fovea, where it merges with the external limiting membrane. This connection is referred to as the Müller cap. ILM peeling, or the removal of the ILM using microsurgical instruments, significantly reduces the risk of postoperative epiretinal membrane (ERM) formation [6]. The procedure of peeling the ILM is also performed to prevent cellular proliferation on its surface and to counteract the development of excessive traction forces [4, 7, 8].
INDICATIONS FOR PEELING
ILM peeling is indicated in various medical conditions as it enhances the regenerative capacity and functionality of the retina. It is commonly used in macular hole (MH) cases to increase the likelihood of closure [3]. The ILM serves as a scaffold for cell proliferation, which can lead to the development of ERM. Peeling is recommended in diseases associated with ERM, including vitreomacular traction syndrome and proliferative diabetic retinopathy [9].
The application of peeling can also yield beneficial effects in iatrogenic or post-traumatic conditions, including chemical or mechanical injuries, as well as following previous ophthalmic procedures [10].
Brilliant blue (BB) dye is increasingly used to visualize the ILM due to its favorable safety profile [11]. BB selectively stains the ILM, but with low contrast. Nonetheless, it is sufficient to visualize the ILM and facilitates its removal by the surgeon [12].
TOOLS USED FOR PEELING
Because ILM peeling requires high precision, it is performed using specialized microsurgical instruments. Forceps allow the ILM to be grasped and removed using the pinch-and-peel technique [13]. This involves directly gripping the membrane and gently pulling it. In some cases, when the pinch-and-peel technique does not facilitate the separation of the ILM, micro-scissors are used to make an incision, making it easier to grasp and remove the membrane [14]. The Tano scraper is a surgical instrument used for the atraumatic peeling of the ILM from the retinal surface during vitrectomy procedures. It features a tip coated with fine diamond particles, which enhances the precision of membrane manipulation while minimizing iatrogenic trauma [15].
To enhance the visibility of the ILM during the procedure, dyes such as indocyanine green (ICG), triamcinolone acetonide (TA), and BB are used [4]. The substance that provides the best visualization of the ILM is TA [16]. Some studies suggest that ICG increases the adverse effects of light on the retina when it is present on its surface. The use of ICG dye in ILM peeling remains controversial, and the results of clinical studies have been mixed. Some studies have shown that ICG-assisted ILM peeling does not worsen visual outcomes or negatively affect retinal function [10, 17]. However, other studies suggest that ICG staining may have an adverse impact on functional outcomes, including less improvement in visual acuity and the development of peripheral visual field defects after surgery [18, 19].
PEELING TECHNIQUES
Techniques used in MH surgery
Pinch-and-peel technique
This traditional method involves grasping and then pulling the ILM to separate the membrane from the retina [4, 20]. Microforceps are the primary tool used for this procedure. In situations where grasping the ILM with forceps is challenging, microscissors can be helpful. This instrument allows for an incision in the ILM, creating a small groove that can then be grasped with forceps [14].
Inverted flap technique
This method, first proposed by Michalewska et al. [21], is used for large or difficult-to-close MHs. Importantly, the described approach may also be employed for ERM removal. It involves detaching the ILM and inverting the flap to cover the MH [4]. The inverted flap acts as a scaffold, supporting cell proliferation and promoting hole closure. Studies have shown that this method improves anatomical outcomes, demonstrating a higher closure rate for MH compared to the pinch-and-peel technique [22].
The inverted ILM flap technique has several modifications. Michalewska et al. [21] suggested a strategy where the Müller membrane in the nasal part of the retina was not peeled, while the flap on the temporal side was detached and placed over the MH. This approach reduced surgical trauma and decreased the incidence of dissociated optic nerve fiber layer (DONFL). Another modification, proposed by Chen [23], uses a large, semicircular ILM flap to cover the MH (Figure 1).
Figure 1
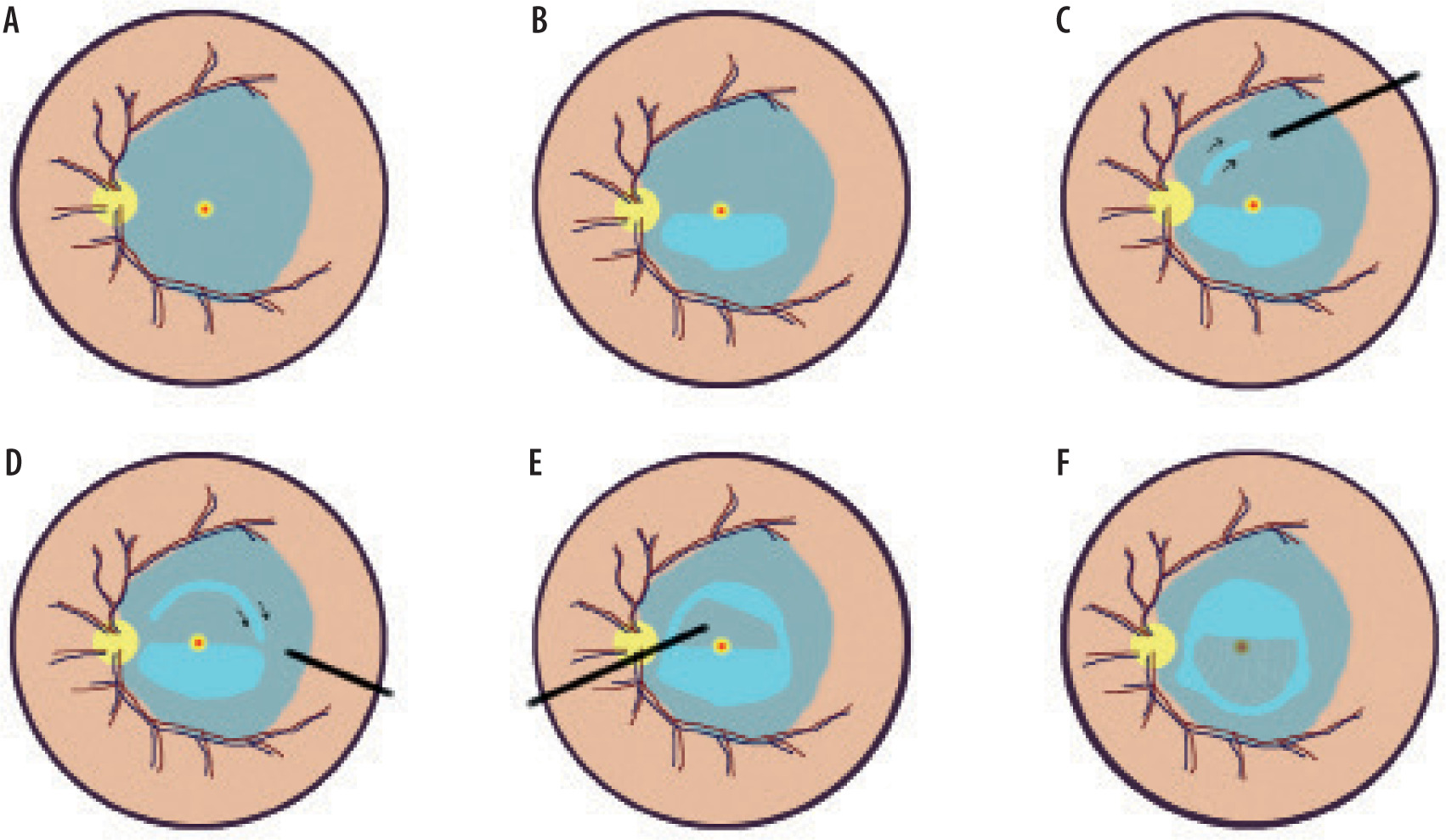
Diagrammatic presentation of the surgical technique for creating a large semicircular internal limiting membrane (ILM) flap: A) The ILM within the vascular arcade is stained with indocyanine green. B) The ILM in the lower macular region is peeled along the vascular arcade toward the edge of the macular hole (MH), covering approximately 180°. C) The ILM is grasped with forceps at the upper (temporal or nasal) part, around two optic disc diameters from the MH, following a circular motion. D) Peeling continues by grasping the edge of the outer ILM tear and progressing circularly. E) After the flap is fully released, it is separated from the retina about 100 µm from the edge of the hole. F) The ILM flap is inverted and placed over the macula [22]
In highly myopic eyes with retinal detachment, a C-shaped inverted ILM flap modification is used [24, 25]. This strategy employs a smaller ILM flap than the classical approach, reducing the risk of complications due to membrane traction. The peeled flap covers 270° rather than the 180° semicircle, facilitating better coverage of the MH.
Aurora et al. [26] performed vitrectomy with ILM peeling based on the cabbage-leaf inverted ILM flap technique. This approach is used to treat full-thickness MH. The method involved creating three inverted ILM flaps, with their bases attached to the edges of the MH. The flaps were trimmed and inverted over the hole, layered similarly to cabbage leaves. The cabbage-leaf technique provided better adherence of the flaps through the connection of the flap’s retinal surface to the vitreous surface [27].
Free ILM flap technique
This technique can be considered for resistant MH after initial surgical failure. Using microforceps, a free ILM flap is harvested from the temporal retina and placed over the MH [28]. This technique is particularly useful when there is insufficient ILM tissue near the hole. Studies suggest similar postoperative physiological and anatomical outcomes between the free ILM flap technique and the inverted ILM flap technique [29].
Multiple free ILM flap implantation technique
The multiple free ILM flap implantation technique was proposed by Chen et al. [30] as a method for patients with small-to-medium MHs and shallow retinal detachment associated with high myopia. The procedure involves removing the ILM, preparing free flaps, and introducing them into the MH using viscoelastic material. This prevents the flaps from floating or migrating into the subretinal space. Multiple flaps are used in this technique, which collectively stabilize within the MH, creating a supporting structure to facilitate hole closure.
Double ILM insertion technique
The double ILM insertion technique was developed to address the limitations of free and inverted ILM flaps in the treatment of large MH and refractory cases after primary surgery, particularly in the context of retinal detachment in high myopia [31]. This technique, introduced by Chen and Yang [32], combines the use of a free ILM flap and an inverted ILM flap, which mutually stabilize their positions within the MH.
Before detaching the ILM, viscoelastic material was applied to prevent ICG dye from entering the MH, thereby reducing dye toxicity. Viscoelastic material was also reapplied after the insertion of the inverted flap, minimizing the risk of displacement. The free ILM flap prevented the inverted flap from collapsing, while the inverted flap held the free flap in place. Through this synergy, the flaps stably filled the MH, supporting its closure [32].
Continuous arcuate peeling
This modern approach to ILM peeling in vitreoretinal surgery is used for large MHs requiring precise membrane removal with minimal retinal trauma. The surgeon initially lifts the membrane with forceps and follows an arcuate trajectory while removing the flaps. This strategy preserves the central macular area, reducing the risk of photoreceptor damage [33].
ILM scraping technique
Caporossi et al. [34] proposed a method where the peeling tool is used to scrape the ILM, simultaneously removing the ERM. At the initial stage of the procedure, the vital dye brilliant blue G is employed to facilitate visualization of the ILM [34]. Subsequently, the surgeon gently strokes the surface of the membrane using the Tano scraper, thereby inducing separation of the ILM from the underlying retina. Once delamination has been achieved, the membrane is removed using the pinch-and-peel technique. The application of the Tano scraper may offer advantages over conventional ILM forceps, particularly in cases where there is an elevated risk of retinal injury during membrane grasping [35].
Techniques used in ERM surgery
Knife-based ILM peeling approach
Walter et al. [20] suggested departing from traditional ILM peeling with forceps by using a loop scraper to separate the membrane. This tool allows a 180° semicircle to be cut along the ILM border, followed by membrane removal with a vitrectomy probe in aspiration mode. This strategy yielded similar functional and anatomical outcomes compared to traditional ILM peeling but significantly reduced surgery time (by approximately 18 minutes). The study suggests an advantage of the forceps-free technique, although this needs to be confirmed by further research.
En bloc ILM peeling technique with ERM
The procedure begins with a pars plana posterior vitrectomy, during which the vitreous body and posterior hyaloid are removed. BB dye is subsequently employed to enhance visualization of the ILM and ERM. Following staining, the surgeon initiates ILM removal using specialized forceps (e.g., Grieshaber DSP 25G) by gently pinching the retinal surface in an area located approximately one optic disc diameter away from the foveal center [36]. The ILM is then progressively delaminated in a tangential direction, creating a broad flap. In the en bloc technique, the ERM and ILM are peeled simultaneously as a single layer, allowing for more effective removal of the pathological structures [37].
BENEFITS
ILM peeling is a surgical procedure primarily used in the treatment of macular disorders, such as MH and ERM [33]. Removing the ILM eliminates tractional forces acting on the edges of the hole, promoting its closure and, consequently, improving visual acuity. ILM peeling minimizes the risk of recurrence of ERM after surgical removal, contributing to the stabilization of retinal function.
Peeling the ILM can lead to better surgical outcomes, including improved visual acuity [38].
POSSIBLE COMPLICATIONS
ILM peeling is an invasive procedure and carries certain risks, such as retinal damage and hemorrhage. The decision to perform the procedure should be made following a thorough assessment of the patient’s condition by an experienced ophthalmologist [39].
Intraoperative complications
Since ILM peeling involves the surgeon applying pressure to the delicate retinal structures, mechanical injuries to the retina can occur [40]. These injuries are typically caused by excessive or perpendicular traction applied to the retina during membrane peeling, leading to the generation of tractional forces. As a result, retinal tears may develop [33].
Tears located on the posterior wall of the retina require laser photocoagulation. For defects in the peripheral retina, a fluid-air exchange followed by fluid-gas exchange combined with laser photocoagulation may be necessary. Tears can also occur when the surgeon inadvertently grasps too much tissue beneath the ILM. A key challenge during ILM peeling is the strong adhesion between the ILM and the underlying structures. Pulling on such tightly adhered membranes may result in superficial retinal hemorrhage or damage to the nerve fiber layer (NFL) [41].
Postoperative complications
The most common postoperative complications include asymptomatic paracentral scotomas, likely associated with mechanical damage to the NFL during ILM peeling [42]. After ILM peeling, the macula often appears whitish with hemorrhages, and swelling resulting from disrupted axonal transport in ganglion cell fibers can lead to the characteristic appearance of DONFL [41, 43]. These changes are typically asymptomatic, although they may sometimes result in micro- scotomas that can affect visual quality.
Functional changes after surgery, such as reduced retinal sensitivity, are usually temporary and do not impact the ultimate improvement in visual acuity. Some studies suggest that ILM peeling may not be necessary for the treatment of small MHs [41].
ICG has been shown to exert a toxic effect on the retina, particularly if injected directly into the eye. Animal and in vitro studies have revealed that ICG has cytotoxic effects on various retinal cell populations, including the retinal pigment epithelium, glial cells, and ganglion cells [44]. These toxins may threaten retinal functionality, especially if the dye spreads underneath the retina.
Despite the potential for complications, ILM peeling is generally safe and effective when performed by an experienced surgeon. The risk of complications can be minimized through proper surgical techniques, the use of appropriate dyes, and diligent postoperative care.
SUMMARY
In summary, ILM peeling has undeniably revolutionized vitreoretinal surgery and significantly advanced the treatment of various retinal disorders, such as MH, ERM, and tractional retinal detachments. Over the years, numerous surgical techniques, ranging from the classic pinch-and-peel method to the inverted ILM flap, and more modern approaches such as scraping and free flap techniques, have not only facilitated the development of effective treatment strategies but also helped identify potential intraoperative and postoperative complications.
ILM peeling remains a cornerstone of modern retinal and macular surgery. Ongoing technological advancements and innovative surgical methods promise to further improve management of complex retinal disorders, enhance therapeutic outcomes, and ultimately benefit patient quality of life.







